
The relationship between quality improvement and performance management
Response by Leslie Beitsch, MD, JD
The relationship between quality improvement (QI) and performance management (PM) is mutually reinforcing. However, sometimes the connection between them is not always so well demarcated. For the past several years, public health leaders have placed great emphasis on embracing QI within their organizations. The Robert Wood Johnson Foundation and the Centers for Disease Control and Prevention have made substantial investments to strengthen public health QI capacity—and through those investments—organizational performance. To contrast, PM has received much less emphasis until recently. Fortunately for public health, more attention is now being directed toward PM.
Readers of this blog are well acquainted with QI, but many of you work in public health organizations that may not yet have fully matured PM systems. First, a quick informal definition: PM is the enterprise-wide effort to harness the power of all the organizational quality initiatives taking place and to align them to achieve strategic priorities. Also known as “Big QI,” PM is within the purview of leadership to establish parameters and guide the system. Some PM systems you are already familiar with are the Turning Point Performance Management Model, Baldrige, and Balanced Scorecard, among others. All are heavily dependent upon QI activities (“Little QI”) occurring within programs and processes (see the definition of public health QI: Riley, Moran, Corso, Beitsch, Bialek, Cofsky. Defining Quality Improvement in Public Health. Journal of Public Health Management & Practice (2010) Vol. 16, Issue 1: 5–7). QI should be guided by Those on the front lines of public health service delivery. Coupled with PM, both top-down and bottom-up philosophies operate concurrently. PM seeks to choreograph these efforts so they add maximal value—rather than risk them becoming random acts of QI. PM cuts across organizational silos and creates value for the entire public health agency by emphasizing those QI activities that are of highest priority and alignment with strategic objectives (see Figure 1).

Figure 1.
One of the major drivers for health departments adopting PM is the recent development of the Public Health Accreditation Board (PHAB) standards, which apply to state, local, and tribal health departments. These consensus standards underscore the interdependent relationship between QI and PM. Within Domain 9 (Evaluate and Continuously Improve Health Department Processes, Programs, and Interventions) are two standards. Standard 9.1 (Use a Performance Management System to Monitor Achievement of Organizational Objectives) and Standard 9.2 (Develop and Implement Quality Improvement Processes Integrated into Organizational Practice, Programs, Processes, and Interventions), taken together, encompass PM and QI. To meet PHAB standards, applicant health departments must provide evidence that they have taken meaningful steps toward implementing PM and conducting routine QI activities.
I am frequently asked, “Do I begin with QI or PM?” The answer I give is, “Yes—please start!” However, where you should begin is heavily dependent upon your health department and its strengths (where you are with respect to QI). Nonetheless, the most important concept is, “Just start!”—my variation on the omnipresent Nike ad. Figure 2 shows the Möbius strip reflecting the QI/PM continuum. Note that it is a seamless pathway, with no obvious entrance or exit. Moreover, to the dismay of some, it is in the shape of the infinity symbol, emphasizing the ongoing, iterative nature of QI/PM. The QI/PM continuum displays quality across multiple dimensions: QI of the organization (Big QI), QI for the program or process (Little QI), and individual QI (how we develop our skills to perform our jobs better). All are present and functioning in a developed PM system, and all include multiple feedback loops to one another. In short, QI and PM are two sides of the same coin and are the indispensable currency required for strengthening public health organizational performance.
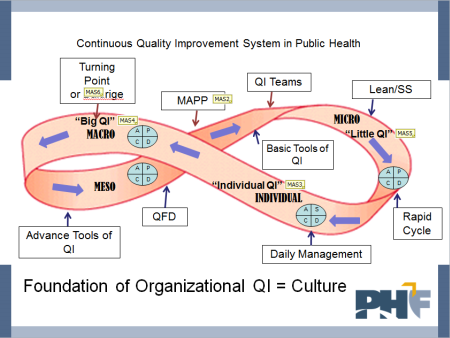
Figure 2.